
Retina/Vitreous Conditions
Flashes and Floaters

Diagram of fluid shift in the eye and detachment of the Vitreous.
Flashes and floaters could be a sign of a Posterior Vitreous Detachment (PVD) or a retinal tear. The vitreous is the clear gelly that fills the center of the eyeball. It is made of water and protein with the consistency of egg white. As we age, the protein structure breaks down and clumps of protein are seen as "floaters."
The vitreous may degenerate to the point where it separates from the eye wall. This is called a Posterior Vitreous Detachment (PVD). A PVD usually does not cause any problems. However, sometimes as the vitreous separates from the retina it may tug and cause a tear. This tugging on the retina causes flashes of light to be seen. Seeing flashes of light does not mean that one has a retinal tear, but it is a worrisome sign. If a retinal tear is detected early it can be treated with laser in the office. However, a tear may progress to retinal detachment at which point more extensive treatment is needed.
Whenever one sees a sudden onset of floater with or without flashes, an eye examination should be sought to rule out a retinal tear.
Diabetic Retinopathy
Diabetic retinopathy is the leading cause of blindess in working age adults in the United States. Diabetes affects several major systems in the body. It can cause kidney failure, nerve damage, and vascular damage. It increases the risk of heart disease and stroke.
The effect of diabetes on the eye is generally classified as non-proliferative and proliferative retinopathy. Non-proliferative diabetic retinopathy affects vision by causing swelling of the retina (macular edema). Macular edema disrupts the function of the retina and leads to vision loss. Macular edema is treated by intraocular injections of “anti-VEGF” medication, laser, and sometime surgery. Prior to treatment, the extent of edema will be assessed by optical coherence tomography and/or fluorescein angiogram. Lucentis, Eylea, and Avastin are the medications commonly injected for treatment, and these are injected in the office with local anesthesia. Sometimes this is used in conjunction with laser treatment and sometimes laser is used by itself. Steroids are also used when the edema does not resolve with these other treatments, most often by injection into the back of the eye. Several different steroids, and steroid implants, may be used. Surgery to remove the vitreous (vitrectomy) may be considered when the edema does not resolve with any of these treatments.


Macular Edema in a Diabetic Patient
Proliferative diabetic retinopathy affects vision by causing bleeding inside the eye (vitreous hemorrhage) or retinal detachment. Abnormal blood vessels grow out of the retina and may break and bleed. This blood in the vitreous can cause sudden severe loss of vision. These abnormal blood vessels may also contract and pull on the retina and cause a tractional retinal detachment. Retinal detachment may also cause devastating loss of vision. The best time to treat Proliferative Diabetic Retinopathy (PDR) is at the early stage when abnormal vessels just start to grow. Treatment is performed with laser in the office. If bleeding or retinal detachment is encountered a vitrectomy may be needed.
Vitrectomy is a procedure performed in the operating room where specialized equipment is used to remove the blood from the eye and remove the membranes that have pulled and detached the retina.
The importance of regular dilated eye examinations for people with diabetes can not be stressed enough. It is best to catch the disease at an early stage and slow any progression than try to fix the damages after the fact. Controlling ones blood sugar and blood pressure is also very important in slowing down the progression of any retinopathy.
Age-related Macular Degeneration (AMD)
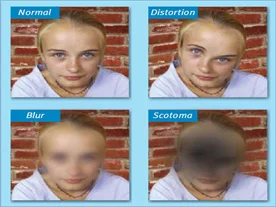
Age-related Macular Degeneration (AMD) is the number one cause of vision loss in people over age 65 years in the U.S. The macula is the part of the retina that is responsible for central vision. Proper macular function is essential for reading and driving. There are two types of AMD: Dry (non-exudative) and Wet (exudative).
Dry AMD is the most common type. In the macula there are characteristic deposits called Drusen. It is believed that drusen may lead to loss, or "atrophy," of the layer beneath the retina (the RPE) which provides nutrients to the retina. Once an area atrophies the overlying retina does not function well and may lead to a blind spot (Scotoma.) If the blind spot is directly in the center it could interfere with reading, recognizing faces, or driving. If it causes a severe loss of vision to worse than 20/200 line on the eye chart, the person is considered legally blind.
Most people diagnosed with AMD have the dry form. Dry AMD progresses slowly. However, it can go onto to the Wet form.
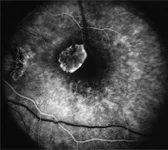
Leaking Blood vessels in an eye with Wet AMD
Wet AMD accounts for most of the vision loss from AMD. In the wet form, abnormal blood vessels grow under the retina and leak or bleed. This causes a sudden change in vision. Sometimes the patient notices that straight lines have a bend in them. Other times a person may notice a blank spot or blurring in vision.
The treatment for Wet AMD is intravitreal injection of anti-VEGF medication. There are several different medications available, all of which are very effective at preventing further vision loss. Your doctor will help determine the best treatment for you. Other treatments that have been used in the past include laser photocoagulation and Photodynamic Therapy with Visudyne. These treatments are rarely used and, overall, are not as effective as intravitreal anti-VEGF therapy.
Posterior Vitreous Detachment (PVD)

Diagram of fluid shift in the eye and detachment of the Vitreous
Flashes and floaters could be a sign of a Posterior Vitreous Detachment (PVD) or a retinal tear. The vitreous is the clear gelly that fills the center of the eyeball. It is made of water and protein with the consistency of egg white. As we age, the protein structure breaks down and clumps of protein are seen as "floaters."
The vitreous may degenerate to the point where it separates from the eye wall. This is called a Posterior Vitreous Detachment (PVD). A PVD usually does not cause any problems. However, sometimes as the vitreous separates from the retina it may tug and cause a tear. This tugging on the retina causes flashes of light to be seen. Seeing flashes of light does not mean that one has a retinal tear, but it is a worrisome sign. If a retinal tear is detected early it can be treated with laser in the office. However, a tear may progress to retinal detachment at which point more extensive treatment is needed.
Whenever one sees a sudden onset of floater with or without flashes, an eye examination should be sought to rule out a retinal tear.
Retinal Tears & Detachment

Retinal tears occur when a posterior vitreous detachment (PVD) leads to pulling and then tearing of the retina. The tear then may allow fluid to get under the retina and cause a detachment.
Posterior Vitreous Detachment (PVD) is when the vitreous separates from the retina.The vitreous is the clear gelly that fills the center of the eyeball. It is made of water and protein with the consistency of egg white. As we age, the protein structure breaks down and clumps of protein are seen as "floaters."
The vitreous may degenerate to the point where it separates from the eye wall. This is called a Posterior Vitreous Detachment (PVD). A PVD usually does not cause any problems. However, sometimes as the vitreous separates from the retina it may tug and cause a tear. This tugging on the retina causes flashes of light to be seen. Seeing flashes of light does not mean that one has a retinal tear, but it is a worrisome sign.
If a retinal tear is detected early it can be treated with laser in the office. However, a tear may progress to retinal detachment at which point more extensive treatment is needed.
Whenever one sees a sudden onset of floater with or without flashes, an eye examination should be sought to rule out a retinal tear.
Uveitis
Uveitis is the inflammation of eye. It may affect the front (anterior uveitis), middle (intermediate uveitis), or the back (posterior uveitis) of the eye.
The most common causes of uveitis include Sarcoidosis, Syphyllis, Tuberculosis, and Inflammatory joint diseases (eg. Reiter's and Behcets Syndromes). In more than half the cases, however, an underlying etiology is not found.
Symptoms of uveitis may include: reduced vision, red eyes, eye pain, and sensitivity to light. Oral therapies include antibiotics, steroids, or chemotherapy. Topical therapyusually involvessteroid and dilating eye drops.
The type of treatment used depends on the level and severity of uveitis and is determined by your physician.
Macular Hole
Macular holes occur right in the center of the macula. In most cases no underlying cause is found although in the younger age-group trauma is the leading etiology. Macular holes are classified in different stages as they evolve from a small defect in the center of the macula to a full-blown hole.
In its early stages it is possible for a macular hole to regress spontaneously. However when the hole fully opens the only effective treatment is vitrectomy. During the operation a membrane (Internal Limiting Membrane) that surrounds the hole is removed and a special gas (c3F8 or SF6) is placed in the eye. The gas serves as a tamponade, keeping the hole sealed as it heals. It is important for the patient to remain face-down after the operation for at least 7-10 days. This allows the gas bubble to prevent the hole from opening again.
It is important for the patient to remain face-down after the operation for at least 7-10 days. This allows the gas bubble to prevent the hole from opening again.
Macular Pucker (Epiretinal Membrane)
Macular pucker, also known as epiretinal membrane, is caused by a membrane growing on the surface of the retina and causing wrinkling of the macular anatomy. It may cause blurry vision or distortion.
The cause of epiretinal membrane formation is not known. It usually does not progress very rapidly. However, if it causes loss of vision vitrectomy surgery with membrane peeling may be warranted. During the surgery the membrane is engaged and peeled off the surface of the retina. In most cases the normal smooth surface of the macula is restored and vision improves. As with all surgeries there is a potential for complications such as infection, bleeding, retinal detachment, or further loss of vision.
Retinal Macroaneurysm
Retunal Macroaneurysm is a rare disorder due to a malformation in a retinal artery. It is oftern associated with high blood pressure. In most cases the aneurysm is a coincidental finding on routine examination and is just observed.
At times the aneurysm may cause bleeding or leaking of fluid. This may lead to loss of vision. Often the aneurysm is treated with laser treatment in the office and the blood resolves. In most cases when the blood resolves there is some improvement in vision. In certain cases when the blood involves the fovea or is not clearing quickly, the retinal surgeon may try to remove the blood by vitrectomy.
The mode of treatment depends on the extent and location of the bleeding.
Branch Retinal Vein Occlusion

Branch Retinal Vein Occlusion (BRVO) is a commonly seen retina problem. The exact cause of this is not known. It is postulated that insites where arteries cross veins a hardened artery may press on the vein below and cause it to close. This condition is most commonly seen in people with high blood pressure, diabetes, cardiovascular problems, or hypercoagulable condition. When the vein closes, the blood that would be returning toward the heart from the retina has no place to go. It then leaks out of the vein and causes bleeding within the retina.The bleeding and leakage from the vessels may then lead to loss of vision. Many cases of BRVO improve on their own; however, treatment with intraocular medication and/or laser can often help those that do not.
Central Retinal Vein Occlusion (CRVO)

Retina with CRVO
Central Retinal Vein Occlusion (CRVO) can cause devastating sudden loss of vision when the central retinal vein, which drains the blood out of the retina, becomes clogged. This causes a back flow of blood and serum which causes the blood to leak into the retina and cause swelling.
There are two types of CRVO: ischemic and non-ischemic. The "ischemia" refers to cases where the flow of blood has been compromised in the arterioles as well and thus parts of the retina are not receiving blood. The disctintion between ischemic and non-ischemic is based on findings on a fluorescein angiogram. Both types of CRVO may have swelling in the center of vision called macular edema. This is often treated with intraocular injection of anti-VEGF (Lucentis, Eylea, or Avastin) or steroid medications. Many patients with non-ischemic macular edema will recover vision through these treatments. Eyes with ischemic CRVO usually have worse vision and are more likely to go on to having complications. The main complication is the growth of new abnormal blood vessels (neovascularization) which may clog the outflow path of eye fluids and cause high pressure. This high pressure may cause the eye to lose further vision and become painful. Patients with CRVO are typically followed monthly for the first few months to check for development of neovascularization. These new vessels are first noticed on the iris. In these cases, patients will often receive pan-retinal laser photocoagulation in addition to anti-VEGF injection. Sometimes vitrectomy or glaucoma surgery becomes necessary as well
Central Serous Retinopathy (CSR)
Central Serous Retinopathy (CSR) is most commonly seen in middle-aged type A (stressed) males. CSR usually cause a moderate loss of vision (20/40 - 20/80) although more severe vision loss may be seen. Some patients complain of a central blind spot (scotoma) or waviness to straight lines (metamorphopsia). The diagosis is definitvely made with fluorescein angiography.
In most case vision returns to close to normal after 3-6 months. Few cases may go on to developing abnormal vessels (choroidal neovascularization) which may require laser treatment.
Patients often want to know if there is any treatment to make the vision return faster. Light laser treatment to the area of leakage may lead to faster recovery but no improvement in final outcome. Similarly use of the oral drugs acetazolamide or spironolactone may return vision a little faster but does not affect the final outcome. Systemic steroid treatment is contraindicated.